Map 109 Kentucky PDF Template
Map 109 Kentucky PDF Template
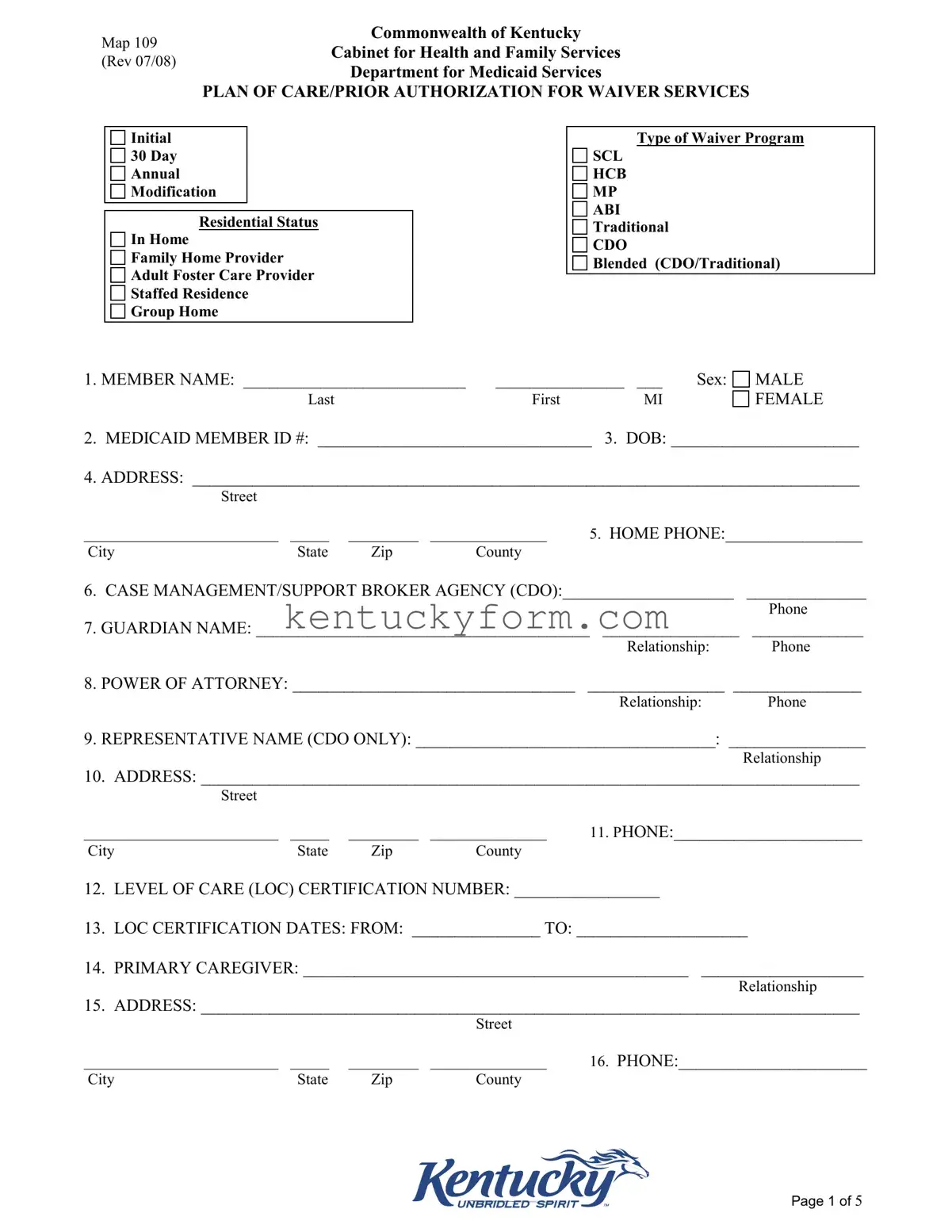
Embarking on a journey through the labyrinth of healthcare and assistance services can often feel overwhelming for both individuals and their families. At the heart of navigating this complex terrain in Kentucky is the Map 109 form, a cornerstone document designed by the Commonwealth of Kentucky Cabinet for Health and Family Services. Revised in July 2008, it serves a pivotal role, acting as a Plan of Care/Prior Authorization for Waiver Services. This essential form is the blueprint for various waiver programs, including SCL, HCB, MP, ABI, Traditional, CDO, and the innovative Blended approach. It meticulously gathers critical member information, from basic identifiers like name, Medicaid ID, and residential status, to more intricate details about the care recipient's needs, their desired outcomes, and the meticulously planned services meant to achieve these goals. Furthermore, it facilitates a harmonious link between care providers and beneficiaries, ensuring a tailored care approach that aligns with the individual's unique circumstances. Whether it's for an initial request, a yearly update, or a necessary modification to the care plan, the Map 109 form stands as a vital tool in the orchestration of personalized, need-based waiver services across Kentucky, aiming to enhance the quality of life for those it serves.
Map 109
Commonwealth of Kentucky
Cabinet for Health and Family Services
(Rev 07/08)
Department for Medicaid Services
PLAN OF CARE/PRIOR AUTHORIZATION FOR WAIVER SERVICES
Initial
30Day Annual Modification
Residential Status
In Home
Family Home Provider
Adult Foster Care Provider
Staffed Residence
Group Home
Type of Waiver Program
SCL
HCB
MP
ABI Traditional
CDO
Blended (CDO/Traditional)
1. MEMBER NAME: __________________________ |
_______________ |
___ |
Sex: |
Last |
First |
MI |
|
MALE
FEMALE
2. MEDICAID MEMBER ID #: ________________________________ 3. DOB: ______________________
4.ADDRESS: ______________________________________________________________________________
Street
_________________________ |
_____ |
_________ |
_______________ |
5. HOME PHONE:________________ |
City |
State |
Zip |
County |
|
6.CASE MANAGEMENT/SUPPORT BROKER AGENCY (CDO):____________________ ______________
Phone
7.GUARDIAN NAME: _______________________________________ ________________ _____________
Relationship: Phone
8.POWER OF ATTORNEY: _________________________________ ________________ _______________
Relationship: Phone
9.REPRESENTATIVE NAME (CDO ONLY): ___________________________________: ________________
Relationship
10.ADDRESS: _____________________________________________________________________________
Street
_________________________ |
_____ |
_________ |
_______________ |
11. PHONE:______________________ |
City |
State |
Zip |
County |
|
12.LEVEL OF CARE (LOC) CERTIFICATION NUMBER: _________________
13.LOC CERTIFICATION DATES: FROM: _______________ TO: ____________________
14.PRIMARY CAREGIVER: _____________________________________________ ___________________
Relationship
15.ADDRESS: _____________________________________________________________________________
Street
_________________________ |
_____ |
_________ |
_______________ |
16. PHONE:______________________ |
City |
State |
Zip |
County |
|
Page 1 of 5

Map 109
Commonwealth of Kentucky
Cabinet for Health and Family Services
(Rev 07/08)
Department for Medicaid Services
PLAN OF CARE/PRIOR AUTHORIZATION FOR WAIVER SERVICES
Member Name: _____________________________ Medicaid Member ID#:__________________________
Identification of Needs/Outcomes/Services/Providers
NEED(S) |
OUTCOMES/GOAL(S) |
OBJECTIVES/INTERVENTION(S) |
SERVICE |
PROVIDER NAME/# |
|
|
|
CODE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 2 of 5
Map 109
Commonwealth of Kentucky
Cabinet for Health and Family Services
(Rev 07/08)
Department for Medicaid Services
PLAN OF CARE/PRIOR AUTHORIZATION FOR WAIVER SERVICES
Member Name: ____________________________________ Medicaid Member ID#: ____________________ Date Services Start: ___________
Support Spending Plan
Traditional Waiver Services
Service Code
A
Provider Name and Number
B
Units per
Week
C
Units per
Month
D
Cost per
Unit
E
Cost per Week (Column CxE)
F
Total Cost Monthly
(4.6xColumn F)
G
Total Cost per Month





 $
$
Consumer Directed Services
|
Service |
Description of Service |
Employee |
Units |
|
Units per |
Hourly |
Number of |
Sum of |
Administrative |
Total |
|
Code |
B |
Providing the |
per |
|
Month (Column |
Wage |
Hours per |
Wages Times |
Costs |
Monthly |
|
A |
|
Service |
week |
|
D x 4.6) |
F |
Month |
Hours |
I |
Amount |
|
|
|
C |
D |
|
E |
|
G |
H |
|
J |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Total Cost |
|
|
|
|
|
|
|
|
|
|
|
Per Month |
|
|
|
|
|
|
|
|
|
|
|
$ |
Page 3 of 5
Map 109
Commonwealth of Kentucky
Cabinet for Health and Family Services
(Rev 07/08)
Department for Medicaid Services
PLAN OF CARE/PRIOR AUTHORIZATION FOR WAIVER SERVICES
Member Name: ______________________________________ Medicaid Member ID #: ______________________
List each provider/employee name, address and telephone number:
Provider/Employee Name
Provider Number Address
Phone Number
Clinical Summary:
_______________________________________________________________________________________________
________________________________________________________________________________________________
_______________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
______________________________________________________________________________________________
Page 4 of 5

Map 109
Commonwealth of Kentucky
Cabinet for Health and Family Services
(Rev 07/08)
Department for Medicaid Services
PLAN OF CARE/PRIOR AUTHORIZATION FOR WAIVER SERVICES
Member Name: _______________________________________________ Medicaid Member ID #: ________________________
Emergency
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
I certify the information contained above is accurate and that I have made an informed choice when selecting the providers/employees to provide each service.
_______________________________________________________________ |
________________________ |
Member/Guardian Signature |
Date |
_______________________________________________________________ |
________________________ |
Case Manager/Support Broker Signature |
Date |
_______________________________________________________________ |
__________________ |
Representative Signature (CDO) |
Date |
Plan of Care/Support Spending Plan
Approved
Denied
_______________________________________________________________ |
__________________ |
QIO Signature/Title |
Date |
Page 5 of 5
| Fact | Detail |
|---|---|
| Purpose | The form is used for creating a Plan of Care/Prior Authorization for Waiver Services for Medicaid services in Kentucky. |
| Scope | It addresses various waiver programs such as SCL, HCB, MP, ABI, Traditional CDO, and Blended (CDO/Traditional). |
| Content | Includes personal information, waiver service plans, provider details, and clinical summaries. |
| Sections | Divided into initial setup, identification of needs/outcomes/services, support spending plan, provider details, clinical summary, and emergency back-up plan. |
| Governing Law | Managed by the Commonwealth of Kentucky Cabinet for Health and Family Services, specifically under the Department for Medicaid Services. |
Filling out the Map 109 Kentucky form is an essential step for accessing certain waiver services through the Commonwealth of Kentucky Cabinet for Health and Family Services. It meticulously records the plan of care or prior authorization needed for waiver services. Approaching this form with a detailed eye ensures that all parties have a clear understanding of the required information, thereby facilitating smoother processing and implementation of the necessary services. By following step-by-step instructions, individuals can accurately complete the form to move forward in securing the support and services they need.
Once the Map 109 form is completed and submitted, it is reviewed by the designated authorities within the Department for Medicaid Services. Approval is necessary for the initiated services to be rendered. Careful adherence to the step-by-step instructions ensures that all relevant information is accurately captured, paving the way for a streamlined review and approval process. The individuals involved can then expect to be contacted about the status of their submission and receive guidance on the next steps towards accessing the necessary waiver services.
Welcome to the detailed FAQ section about the Map 109 Kentucky form. This guide is designed to help individuals understand and fill out the Map 109 Commonwealth of Kentucky Cabinet for Health and Family Services form, required for the Plan of Care/Prior Authorization for Waiver Services.
What is the Map 109 form and who must complete it?
The Map 109 form is a document issued by the Commonwealth of Kentucky Cabinet for Health and Family Services, specifically by the Department for Medicaid Services. It's used for establishing a Plan of Care or obtaining Prior Authorization for Waiver Services for Medicaid members. It needs to be completed by Medicaid members in Kentucky who are entering, residing in, or modifying their care within certain waiver programs such as SCL, HCB, MP, ABI, Traditional, CDO, or a blended program.
Which types of waiver programs are eligible for the Map 109 form?
Eligible waiver programs include Support for Community Living (SCL), Home and Community Based (HCB), Michelle P. Waiver (MP), Acquired Brain Injury (ABI), Traditional, Consumer Directed Option (CDO), and Blended programs. This form is crucial for participants in these programs to authorize services or establish their care plans.
How frequently must the Map 109 form be updated or revised?
The Map 109 form must be updated or revised whenever there's an initial request for services, at 30-day intervals, annually, or when any modification to the Plan of Care is necessary. These updates ensure that the member’s needs are accurately reflected and met according to their current status.
Who is responsible for ensuring the accuracy of the information on the Map 109 form?
Both the member (or their guardian) and their case manager or support broker are responsible for ensuring that the information provided on the Map 109 form is accurate and truthful. Accurate information is crucial for the proper execution and approval of the care plan or services needed.
What information about the member is needed to complete the Map 109 form?
Member-related information required includes their full name, Medicaid Member ID, date of birth, address, home phone number, and residential status. It also requires details about the primary caregiver, guardian, or power of attorney, if applicable. This comprehensive data helps in strategic planning and service allocation tailored to the member’s needs.
What should be done if a member’s circumstances change after the Map 109 form has been submitted?
If the member’s circumstances change, a modification request should be submitted using the Map 109 form to reflect the new information or needs. Timely updates can facilitate adjustments in services or care plans to better suit the member's requirements.
What is the importance of the Level of Care (LOC) Certification Number on the Map 109 form?
The Level of Care (LOC) Certification Number is crucial as it verifies the member's eligibility for waiver services based on their medical and support needs. This number, along with the certification dates, ensures that members receive appropriate services under the Medicaid program.
Can the Map 109 form be completed and submitted online?
Instructions for submission methods, including whether the Map 109 can be completed and submitted online, typically depend on state and program-specific guidelines. It's advised to consult directly with a case manager or the Department for Medicaid Services for the most current process.
Where can additional assistance be found if there are questions or difficulties completing the Map 109 form?
For additional assistance, contact the Department for Medicaid Services or a case manager. They can provide guidance, answer questions, and help navigate through the process of completing and submitting the Map 109 form.
Filling out the Map 109 Kentucky form, which is essential for receiving waiver services, often entails complexities that users might overlook. Common errors can lead to delays or denials in service authorization. By understanding and avoiding these errors, applicants can ensure a smoother process.
One common mistake is incomplete information. Users sometimes leave sections blank because they're unsure of the answer or because they think it’s not applicable to their situation. Every field, unless explicitly stated as optional, must be filled out to avoid processing delays. Particularly, personal details like the Medicaid Member ID# and DOB (Date of Birth) are critical for identifying the applicant within the system.
Another area often mishandled is the identification of needs and the corresponding services to meet those needs. Applicants should work closely with their healthcare providers to accurately pinpoint and articulate these requirements. Moreover, underlying services and projected outcomes must align with the individual's specific circumstances and goals. Misalignment here can lead to services that don't adequately address the member's needs or, worse, the denial of beneficial services.
In conclusion, paying close attention to detail and working collaboratively with knowledgeable individuals can mitigate most mistakes made on the Map 109 Kentucky form. Ensuring that all information is accurate, complete, and fully understood before submission is crucial for a smooth process. Recognizing and addressing common pitfalls increases the likelihood of receiving timely and appropriate waiver services.
The Map 109 Kentucky form is a critical document within the realm of Medicaid services, specifically tailored for those who require plans of care or prior authorization for waiver services in Kentucky. In the execution of this form, various additional documents frequently come into play to ensure a comprehensive and accurate care plan is developed. These documents, ranging from personal identification to clinical assessments, are indispensable in assembling a detailed blueprint for patient care.
Together, these documents contribute to a well-rounded plan of care, ensuring that both the care providers and the members are well-informed and prepared for the services outlined in the Map 109 form. By integrating these forms and documents with the Map 109 Kentucky form, it ensures a holistic approach to care planning and authorization, tailored to the specific needs and circumstances of Medicaid members in Kentucky.
The Advance Directive document, similar to the Map 109 Kentucky form, outlines a person's preferences for medical care if they become unable to make decisions for themselves. This form’s structure, focusing on future medical services and care preferences, parallels the Plan of Care/Prior Authorization sections of the Map 109, which detail the services and care coordination for an individual under certain health programs. Both documents serve to guide healthcare providers and ensure the individuals’ healthcare wishes are understood and considered.
A Power of Attorney document, highlighting parallels with the Map 109 form, designates someone to make decisions on another's behalf. This similarity is evident in the Map 109 sections that request Power of Attorney and Guardian information, offering a legal framework for decision-making authority, especially related to healthcare and welfare services under the specified waiver programs. Both documents establish a represented decision-making process, emphasizing the importance of authorized individuals in healthcare planning and coordination.
The Guardianship Agreement, comparable to sections within the Map 109 form, formalizes an individual’s responsibility to care for someone who is unable to care for themselves. The Map 109’s focus on identifying guardians and representatives aligns with the goal of a Guardianship Agreement to ensure safe and proper care, mirroring the intent to protect and manage the welfare of individuals needing assistance with decision-making or healthcare services.
Service Plan documents, like those found within the realm of personal care services, share similarities with the Map 109 form by outlining the specific services an individual requires. These plans often include detailed descriptions of needed services, allocated providers, and anticipated outcomes, closely resembling the Map 109’s comprehensive breakdown of needs, goals, interventions, and provider information, all aimed at tailoring services to meet the individual’s healthcare objectives.
Prior Authorization Request forms required by insurance companies or Medicaid, analogous to the Map 109 form, are necessary for approval before receiving certain healthcare services or medications. The structure and purpose of the Map 109 closely match these documents, as it includes a section for prior authorizations for waiver services, ensuring that the services planned are covered and pre-approved to avoid unnecessary healthcare expenses.
The Individualized Education Program (IEP), though primarily an educational tool, shares a fundamental similarity with the Map 109 Kentucky form in its structured approach to planning and documenting individualized services. Both documents aim to assess needs, set objectives, and monitor the provision and efficiency of personalized programs, whether they are for educational or healthcare services, emphasizing a tailored approach to support the individual's unique requirements.
The Individualized Service Plan (ISP) utilized in various care settings, including developmental disability and elder care, closely mirrors the Map 109 form. Each document focuses on personalized care coordination, detailing service agreements, care providers, and specific outcomes expected, showcasing how personalized plans operate across different sectors to ensure comprehensive support tailored to individual needs.
The Residential Lease Agreement, while primarily a contract for housing, shares some parallels with aspects of the Map 109 form, specifically in sections detailing Residential Status and Provider information. Both documents address arrangements concerning where and with whom individuals will live, though in different contexts, emphasizing the importance of documented agreements in securing stable and appropriate living situations.
The Medical History Form, like the Map 109, collects vital health information for use in planning and providing care. Although serving more general purposes, both documents compile essential data that informs care decisions, from past medical treatments to current health needs, ensuring that healthcare providers have a comprehensive understanding of the individual’s health background for informed care planning.
Finally, the Emergency Contact Form, akin to the emergency backup plan section in the Map 109 Kentucky form, provides crucial information for unexpected situations. Both documents underscore the necessity of having readily accessible contact information and predetermined plans to ensure safety and continuity of care during emergencies, highlighting preparedness as a key component of care planning.
When completing the MAP 109 Kentucky form for Plan of Care/Prior Authorization for Waiver Services, navigating the details accurately is crucial. Below are guidelines to help ensure the process is smooth and the application is correctly filled out.
Things You Should Do:
Things You Shouldn't Do:
Understanding the complexities of the Map 109 form used within Kentucky's Medicaid services can be challenging. There are common misconceptions surrounding this document, specifically its purpose and application. Here, we address five of these misconceptions to provide clearer insights.
By addressing these misconceptions, individuals and families navigating Kentucky's Medicaid services can better understand the Map 109 form's purpose and use it effectively to meet their care needs. It's crucial for beneficiaries to have accurate information to navigate their options within Medicaid comprehensively.
Filling out the Map 109 form in Kentucky is crucial for individuals requiring waiver services through Medicaid. Here are some key takeaways to help guide you through the process:
Thoroughly completing the Map 109 form is a step forward in accessing necessary waiver services. It lays the groundwork for receiving care that is attentive to individual needs and circumstances, ensuring Medicaid participants can maintain or improve their quality of life. Remember, reaching out for assistance from a healthcare provider or a Medicaid representative can provide clarification and support throughout this process.
Aoc-856 - Assists guardians or conservators in neatly categorizing financial transactions for ease of understanding and review.
Kentucky Inheritance Tax Return - Refund address and payment information for checks are specified distinctively on the form.